You might also like
- Clinical and Radiographic Assessment of Vital Pulpotomy in Primary Molars Using Mineral Trioxide Aggregate and A Novel Bioactive Cement.Document7 pagesClinical and Radiographic Assessment of Vital Pulpotomy in Primary Molars Using Mineral Trioxide Aggregate and A Novel Bioactive Cement.nidaulfaNo ratings yet
- 7.mineral Trioxide Aggregate and FormocresolDocument6 pages7.mineral Trioxide Aggregate and FormocresolMihaela TuculinaNo ratings yet
- ContempClinDent24296-2652559 072205Document6 pagesContempClinDent24296-2652559 072205Kevin EfriandhaniNo ratings yet
- Pediatric Dental Journal: The Efficacy of Portland Cement As A Pulpotomy Agent in Deciduous TeethDocument7 pagesPediatric Dental Journal: The Efficacy of Portland Cement As A Pulpotomy Agent in Deciduous Teethisti DaristiviaNo ratings yet
- Mineral Trioxide Aggregate and Formocresol Pulpotomy of Primary Teeth: A 2-Year Follow-UpDocument7 pagesMineral Trioxide Aggregate and Formocresol Pulpotomy of Primary Teeth: A 2-Year Follow-UpRifqi Aris PranataNo ratings yet
- The Effect of Mineral Trioxide Aggregate On Dental Pulp Healing in The Infected Pulp by Direct Pulp Capping - 2021 - Xu DDocument7 pagesThe Effect of Mineral Trioxide Aggregate On Dental Pulp Healing in The Infected Pulp by Direct Pulp Capping - 2021 - Xu DMairisa SulfaniNo ratings yet
- Colorful Modern Business Infographic PresentationDocument15 pagesColorful Modern Business Infographic PresentationbbNo ratings yet
- Spectrophotometric Analysis of Coronal Tooth Discoloration Induced by Various Bioceramic Cements and Other Endodontic MaterialsDocument5 pagesSpectrophotometric Analysis of Coronal Tooth Discoloration Induced by Various Bioceramic Cements and Other Endodontic MaterialsKristineNo ratings yet
- 3MIXTATINDocument45 pages3MIXTATINShameena KnNo ratings yet
- Al Rafidain Universiy College of DentistryDocument23 pagesAl Rafidain Universiy College of DentistrymahmoodNo ratings yet
- JC 8Document33 pagesJC 8Ramya PaiNo ratings yet
- MTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Document6 pagesMTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Abdul Rahman AlmishhdanyNo ratings yet
- Apexogenesis of A Symptomatic MolarDocument6 pagesApexogenesis of A Symptomatic Molarkhawla boukhNo ratings yet
- Mineral Trioxide Aggregate Applications in Endodontics: A ReviewDocument9 pagesMineral Trioxide Aggregate Applications in Endodontics: A ReviewKatherine CiezaNo ratings yet
- Comparative in Vitro Assessment of Tooth Color Change Under The Influence of NFC and MtaDocument6 pagesComparative in Vitro Assessment of Tooth Color Change Under The Influence of NFC and MtaAuliaNo ratings yet
- Aminabadi 2016Document8 pagesAminabadi 2016Dina ElkharadlyNo ratings yet
- Pedodontic Lect 18Document6 pagesPedodontic Lect 18Mustafa AmmarNo ratings yet
- Primary Tooth Pulp Therapy - Dr. Elizabeth BerryDocument52 pagesPrimary Tooth Pulp Therapy - Dr. Elizabeth BerryMihaela TuculinaNo ratings yet
- Comparative Study of Pulpal Responses To Pulpotomy With Proroot Mta, Retromta, and Theracal in Dogs' TeethDocument8 pagesComparative Study of Pulpal Responses To Pulpotomy With Proroot Mta, Retromta, and Theracal in Dogs' TeethPaulina ÁlvarezNo ratings yet
- Mta Vs Formocresol PulpotomyDocument4 pagesMta Vs Formocresol PulpotomySitapriya SubrahmanyamNo ratings yet
- Performantele MTA - Docx - enDocument5 pagesPerformantele MTA - Docx - enana aNo ratings yet
- Pulpotomy With PRFDocument8 pagesPulpotomy With PRFSai KalyanNo ratings yet
- Unit 4 Management of Open Pulp in Deciduous TeethDocument11 pagesUnit 4 Management of Open Pulp in Deciduous Teethisti DaristiviaNo ratings yet
- Clinical Trial Pulpotomy Biodentine Vs MtaDocument7 pagesClinical Trial Pulpotomy Biodentine Vs MtagiselaNo ratings yet
- Clinical, Radiographic and Histologic Analysis of The Effects of Pulp Capping Materials Used in Pulpotomies of Human Primary TeethDocument8 pagesClinical, Radiographic and Histologic Analysis of The Effects of Pulp Capping Materials Used in Pulpotomies of Human Primary TeethkoajitoNo ratings yet
- A Randomized Controlled Clinical Trial Comparing Tricalcium Silicate and Formocresol Pulpotomies Followed For Two To Four YearsDocument5 pagesA Randomized Controlled Clinical Trial Comparing Tricalcium Silicate and Formocresol Pulpotomies Followed For Two To Four YearsSalsabila Tri YunitaNo ratings yet
- Alternative - Interventions To FormocrescolDocument9 pagesAlternative - Interventions To FormocrescolAsh PeiNo ratings yet
- "Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Document3 pages"Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Ruchi ShahNo ratings yet
- 4-Year Follow-Up of Full PulpotomyDocument9 pages4-Year Follow-Up of Full PulpotomyAshley MarkNo ratings yet
- Root Reconstructed With Mineral Trioxide Aggregate and Guided Tissue Regeneration in Apical Surgery: A 5-Year Follow-UpDocument5 pagesRoot Reconstructed With Mineral Trioxide Aggregate and Guided Tissue Regeneration in Apical Surgery: A 5-Year Follow-UpKranti PrajapatiNo ratings yet
- Clinical and Radiographic Comparison of Biodentine, Mineral Trioxide Aggregate and Formocresol As Pulpotomy Agents in Primary MolarsDocument8 pagesClinical and Radiographic Comparison of Biodentine, Mineral Trioxide Aggregate and Formocresol As Pulpotomy Agents in Primary MolarsDana StanciuNo ratings yet
- Densitometric Analysis of The Autogenous Demineralized Dentin Matrix On The Dental Socket Wound Healing Process in HumansDocument7 pagesDensitometric Analysis of The Autogenous Demineralized Dentin Matrix On The Dental Socket Wound Healing Process in HumansTiago EscobarNo ratings yet
- Full Mouth Zirconia Based Implant Supported Fixed Dental Prostheses. Five Year - Results of A Clinical Pilot StudyDocument5 pagesFull Mouth Zirconia Based Implant Supported Fixed Dental Prostheses. Five Year - Results of A Clinical Pilot StudyAndres CurraNo ratings yet
- Bicompatibility of Regular and White Mta and A Grey Portland Cement in Human Dental PulpDocument5 pagesBicompatibility of Regular and White Mta and A Grey Portland Cement in Human Dental PulpRista LewiyonahNo ratings yet
- Vital Pulp Theray in Permenant Tooth Kursus Resto FinalDocument55 pagesVital Pulp Theray in Permenant Tooth Kursus Resto FinalAmni AzmiNo ratings yet
- A Review On Vital Pulp Therapy in PrimarDocument10 pagesA Review On Vital Pulp Therapy in PrimarMihaela TuculinaNo ratings yet
- Endodontic Management of An Infected Primary Molar in A Child With Agenesis of The Permanent PremolarDocument4 pagesEndodontic Management of An Infected Primary Molar in A Child With Agenesis of The Permanent PremolarFebriani SerojaNo ratings yet
- Pi Is 0099239917300067Document8 pagesPi Is 0099239917300067Alina AlexandraNo ratings yet
- The Effect of Four Materials On Direct Pulp Capping: An Animal StudyDocument8 pagesThe Effect of Four Materials On Direct Pulp Capping: An Animal StudyjennifertaniaNo ratings yet
- Dr. Vibha Hegde - 18Document5 pagesDr. Vibha Hegde - 18Biswaroop ChandraNo ratings yet
- Long-Term Survival of Indirect Pulp Treatment Performed in Primary and Permanent Teeth With Clinically Diagnosed Deep Carious LesionsDocument4 pagesLong-Term Survival of Indirect Pulp Treatment Performed in Primary and Permanent Teeth With Clinically Diagnosed Deep Carious LesionsBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- IJCPD 15 S80 - CompressedDocument7 pagesIJCPD 15 S80 - Compressedviviana tutasigNo ratings yet
- Apexogenesis and ApexificationDocument4 pagesApexogenesis and ApexificationAlandNovrianDwiSaputraNo ratings yet
- Apexification of Anterior Teeth: A Comparative Evaluation of Mineral Trioxide Aggregate and Calcium Hydroxide PasteDocument6 pagesApexification of Anterior Teeth: A Comparative Evaluation of Mineral Trioxide Aggregate and Calcium Hydroxide PastefatimahNo ratings yet
- Dentinogenic Responses After Direct Pulp Capping of Miniature Swine Teeth With BiodentineDocument5 pagesDentinogenic Responses After Direct Pulp Capping of Miniature Swine Teeth With BiodentineAndreaLagunasNo ratings yet
- Fate of Primary Molar Without Permanent Successor A Twin Case ReportsDocument6 pagesFate of Primary Molar Without Permanent Successor A Twin Case ReportsTJPRC PublicationsNo ratings yet
- Juni Save Root Pulp J LSTR LDocument6 pagesJuni Save Root Pulp J LSTR LAntony SebastianNo ratings yet
- Mini-Implant Supported Canine Retraction With Micro-Osteoperforation: A Split-Mouth Randomized Clinical TrialDocument7 pagesMini-Implant Supported Canine Retraction With Micro-Osteoperforation: A Split-Mouth Randomized Clinical Triallaura velez0% (1)
- Remineralization of Artificial Enamel Lesions by Theobromine PDFDocument7 pagesRemineralization of Artificial Enamel Lesions by Theobromine PDFLjubomirErdoglijaNo ratings yet
- Mineral Trioxide AggregatDocument5 pagesMineral Trioxide AggregatRicho AlristaNo ratings yet
- Usage of White MTA in A Non-Vital Primary Molar With No Permanent SuccessorDocument4 pagesUsage of White MTA in A Non-Vital Primary Molar With No Permanent Successorsümeyra akkoçNo ratings yet
- Biofilm Formation On Dental Implants With Different Surface Micro Topography: An in Vitro StudyDocument10 pagesBiofilm Formation On Dental Implants With Different Surface Micro Topography: An in Vitro StudySofia LondoñoNo ratings yet
- A Z Pulpotomy Agent Literature ReviewDocument8 pagesA Z Pulpotomy Agent Literature ReviewSparklez Dental clinicNo ratings yet
- The Open Dentistry JournalDocument9 pagesThe Open Dentistry JournalpoojaNo ratings yet
- Effects of Chemical Agents On Physical PDocument5 pagesEffects of Chemical Agents On Physical PMihaela TuculinaNo ratings yet
- The Problems Preventing Progress in Adhesive Restorative DentistryDocument6 pagesThe Problems Preventing Progress in Adhesive Restorative DentistrygermanNo ratings yet
- Pediatric Dental JournalDocument6 pagesPediatric Dental JournalAndres RamosNo ratings yet
- Van HeerdenDocument5 pagesVan HeerdendorinkarakogluNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Biologic Width - The No Encroachment Zone: I J D ADocument8 pagesBiologic Width - The No Encroachment Zone: I J D AJinny ShawNo ratings yet
- ChemFil Superior44Document27 pagesChemFil Superior44محمد ابوالمجدNo ratings yet
- Dental Anatomy DecksDocument362 pagesDental Anatomy Decksapi-2629165183% (6)
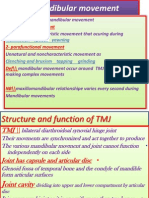
- Mandibular MovementDocument4 pagesMandibular Movementمحمد ابوالمجدNo ratings yet
- VitaminsDocument13 pagesVitaminsمحمد ابوالمجدNo ratings yet
- VitaminsDocument13 pagesVitaminsمحمد ابوالمجدNo ratings yet
- 4 3 937Document4 pages4 3 937محمد ابوالمجدNo ratings yet
- Guidelines On Infection Control in Dental ClinicsDocument10 pagesGuidelines On Infection Control in Dental ClinicsHare RamNo ratings yet
- Anatomy of CNSDocument32 pagesAnatomy of CNSLeonita AguillonNo ratings yet
- Publication PDFDocument28 pagesPublication PDFمحمد ابوالمجدNo ratings yet
- Dental Cements For UseDocument28 pagesDental Cements For UseAhmed DolaNo ratings yet
- Mandibular MovementDocument4 pagesMandibular Movementمحمد ابوالمجدNo ratings yet
- Anatomy of CNSDocument32 pagesAnatomy of CNSLeonita AguillonNo ratings yet
- Publication PDFDocument20 pagesPublication PDFمحمد ابوالمجدNo ratings yet
- Finishing and PolishingDocument18 pagesFinishing and Polishingab0maiNo ratings yet
- Smear LayerDocument9 pagesSmear Layerpriyanka_gedamNo ratings yet
- Anatomy of CNSDocument32 pagesAnatomy of CNSLeonita AguillonNo ratings yet
- Asnan 7 RulesDocument2 pagesAsnan 7 Rulesمحمد ابوالمجدNo ratings yet
- Serial Extraction PedoDocument23 pagesSerial Extraction PedoSelim BaftiuNo ratings yet
- Emergency MedicineDocument7 pagesEmergency Medicineمحمد ابوالمجدNo ratings yet
- 1Document15 pages1محمد ابوالمجدNo ratings yet
- Behaviour Management 2Document59 pagesBehaviour Management 2Nikhil RaiNo ratings yet
- Dental Management of Medically Compromised PatientsDocument12 pagesDental Management of Medically Compromised Patientsمحمد ابوالمجدNo ratings yet
- MCQSeptember 2006 Paper IDocument3 pagesMCQSeptember 2006 Paper Iapi-26291651100% (1)
- MCQPaperSept 05Document4 pagesMCQPaperSept 05api-26291651100% (1)
- Etiology of MalocclusionDocument28 pagesEtiology of MalocclusionPriyaancaHaarsh100% (3)
- Tooth MovementDocument14 pagesTooth Movementمحمد ابوالمجدNo ratings yet
- DentistryDocument71 pagesDentistryAnupama NagrajNo ratings yet
- RO0111 00-00 WebberDocument6 pagesRO0111 00-00 WebberARTNo ratings yet
- OcclusionDocument17 pagesOcclusionمحمد ابوالمجدNo ratings yet